
A decreased lumbar lordosis (hypolordosis) can be best observed when viewing your client from the side. In this posture the normal lumbar curve is lost, flattening the low back, and the pelvis is posteriorly tilted. As mentioned in previous chapters, this posture is sometimes referred to as flatback. A horizontal crease can sometimes be observed in the abdomen when viewing your client from the front. Such as crease can be seen on this patient even in the side view .
There is a tendency for loss of lumbar lordosis in the elderly; as Sparrey and colleagues (2014) describe in their review, surgical management of lumbar posture restores posture at the expense of flexibility and has a high incidence of complications. Finding ways to help patients manage and possibly correct lumbar posture without the need for surgical intervention is likely to be beneficial.
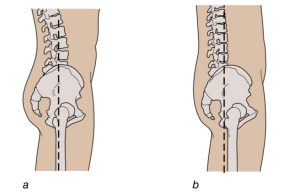 Lumbar spine indicating (a) normal lumbar posture, (b) decreased lumbar lordosis
Lumbar spine indicating (a) normal lumbar posture, (b) decreased lumbar lordosis
Consequences of Decreased Lumbar Lordosis
Although slight flexion of the lumbar spine reduces stress on the apophyseal joints (Adams and Hutton 1980) and compressive force on the posterior annulus, in the hypolordotic posture there is increased compressive stress on the anterior annulus of discs and increased hydrostatic pressure in the nucleus at low load levels (Adams and Hutton 1985). Whether pressure on the anterior portion of discs is harmful in the long term is likely to depend on the disc morphology of individual patients. Scan- nell and McGill (2003) note that a patient with a hypolordotic posture could be at greater risk for strain-related tissue failure than a person with hyperlordosis. Patients with low back pain often have hypolordosis, but it is not clear whether hypolordosis occurs before low back pain or whether these patients flatten their lumbar spines as a pain avoidance mechanism.
What You Can Do as a Therapist
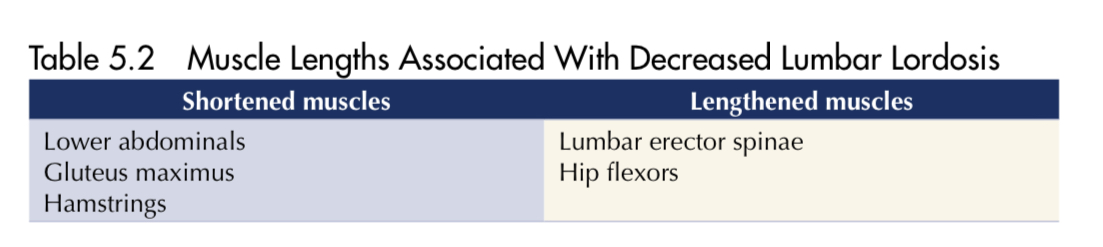
■ Lengthen shortened muscles by applying passive stretches to gluteus maximus and hamstrings .Lengthening of the hamstring muscles has long been advocated for the correction of hypolordosis (Kendall et al. 1993). In their study, Li and colleagues (1996) found no change in lumbopelvic posture after hamstring stretching, but others have questioned some of the methods used in that particular study (Gajdosik 1997). The hamstring stretch shown here is a good starting point for using muscle energy technique.
■ Stretch and lengthen gluteal and hamstring muscles using deep tissue massage. When massaging hamstrings, you could apply strokes using your forearms . You could also use soft tissue technique, locking tissues when they are in a shortened position before passively extending the knee.
■ Treat trigger points in hamstrings and gluteals.
■ In a study by Harrison and colleagues (2002) the application of passive lumbar extension traction increased the lordotic curve in a group of patients with low back pain who had reduced lumbar curves. One and a half years later the follow-up tests revealed that 34 of the 48 participants in the study had retained this improvement. The authors believe that the corresponding decrease in pain reported by patients was the result of the patients’ changed lumbar posture. Whilst useful for research,the apparatus required to provide this traction was large and therefore not a practical treatment for use on a daily basis by most body workers.
■ Tape the lumbar spine to encourage extension.
What Client Can Do
■ Avoid prolonged postures that encourage lumbar flexion. For example, avoid slouched sitting or sitting on low chairs or the floor.
■ Adopt resting postures that encourage extension of the spine. For example, sleeping on the front of the body and resting in the sphinx position or resting on the back with a small firm pillow or a bolster beneath the lumbar spine, is a position similar (though less exaggerated) to the passive traction position used by Harrison and colleagues (2002), which the authors found decreased hypolordosis. Smith and Mell (1987) found that use of the sphinx position for 2 minutes a day for 4 weeks prevented a decrease in passive lumbar extension in male participants but not in females. Their participants were healthy and young, and it would be useful to replicate this experiment on patients with existing hypolordosis.
■ Use of a lumbar support has been advocated to decrease hypolordosis in the sit- ting position (Majeske and Buchanan 1984). Many inexpensive versions of these are widely available and all similar. They are made of soft mesh or foam and attached to the back of a chair with elastic so that they can be moved up or down to suit the user’s posture.
■ Sitting with the chair seat inclined downwards at the front or sitting on a wedge- shaped cushion also increases the lumbar lordosis. It is not known whether the lumbar support, chair tilt position or use of a wedge will affect the posture of a patient with hypolordosis because these are believed to change spine posture in
individuals with normal spines where range of motion is not impaired. However, such devices are worth considering as interventions for the purposes of experimentation.
■ Actively practice extension of the spine. This could be as simple as leaning back whenever possible during the day.
■ Certain physical activities encourage extension of the lumbar spine and could be incorpo- rated into a weekly routine for patients with hypolordotic postures. For example, using a hula hoop requires both flexion and extension of the spine in order to keep the hoop in motion; swimming b in the prone position encourages lumbar extension.
■Strengthen muscles that bring about an anterior pelvic tilt. A case study by Yoo (2013) describes how a patient with flatback was being treated for lumbar pain and given a 2-week programme of daily strengthening exercises for the erector spinae, iliopsoas and rectus femoris, and an increase in pelvic tilt angle was recorded after 2 weeks. Kendall and colleagues (1993) note that one of the challenges inherent to the correction of a hypolordosis is that gluteal muscles tend to be strong and hamstrings short in this posture, and exercises designed to increase lordosis when performed in the prone position activate these hip extensors. Kendall advocates increasing lordosis by raising the legs unilaterally in the prone position, extending the hip by only 10 degrees
■ Lengthen shortened muscles by doing active gluteal and hamstring stretches.
■ Practice walking on an incline. Kim and Yoo (2014) found that in a study of eight participants with flatback syndrome, walking on a treadmill set to a 30-degree incline demonstrated a significant increase in anterior tilt of the pelvis after this activity. Although a protocol for duration and intensity is not established, this study is an example of a simple activity that could be adopted daily in order to determine its effect on hypolordosis.

